Reviewed by: Mr William Sharples BSc (Hons) – Pain Management Expert
Last Updated: September 2025
What are the Stages of Calcific Tendinopathy?
There are three stages of calcific tendonitis:
- Pre-calcific: The initial stage of calcification, with cellular changes. Movement is associated with pain and decreased range of motion.
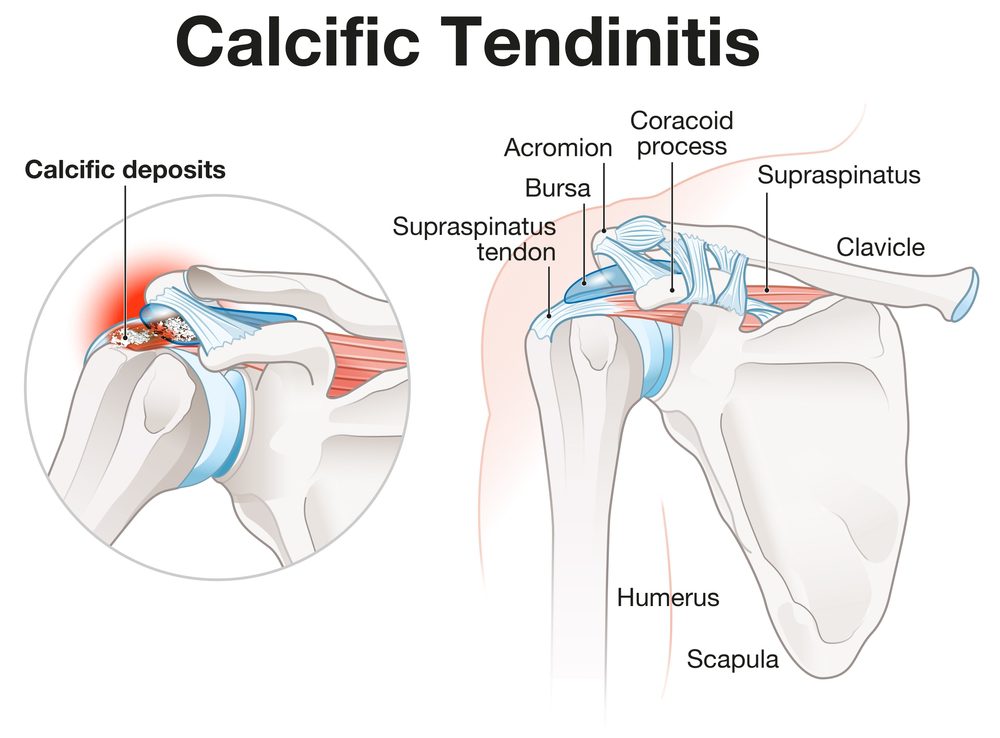
- Calcific: Characterized by calcium buildup (1) inside the cells. The body starts to resorb the calcific deposits. This is the most painful stage.
- Post-calcific: The recovery stage, where calcium deposits are replaced by healthy tendon tissue. Range of movement improves.

Causes of Calcific Tendonitis Shoulder
The exact cause is unknown, but wear and tear of the shoulder is the most common cause. Other associated conditions include:
- Advancing age: Degenerative changes in tendons lead to calcium deposits and chronic calcific shoulder tendinitis.
- Abnormal thyroid activity: The thyroid gland regulates calcium. Dysfunction can elevate calcium levels and promote shoulder calcification.
- Vigorous shoulder movements: Athletes and those with repetitive overhead activity are more prone to tendon damage and pain.
- Genetic predisposition: Family history increases risk.
- Diabetes mellitus: A metabolic disease that increases risk of acute calcific tendinitis and small calcific deposits in soft tissues. (2)
How Does Calcific Tendonitis Occur?
Calcific tendonitis is an inflammatory reaction to calcium deposits in the tendons. When tendons are damaged, calcium salts are deposited, stimulating inflammation. This most often occurs in the shoulder but can affect other areas. Patients may experience pain, swelling, and restricted movement, impacting daily activities. This condition may also contribute to shoulder bursitis (subacromial impingement syndrome) and affect the biceps tendon.
The rotator cuff is a group of tendons around the shoulder, and calcification most often occurs in these tendons (3). The inflammatory response to calcification promotes swelling, pain, and impaired function.
Signs & Symptoms
- Sudden onset of shoulder pain: Due to inflammation and irritation of nerve endings. Pain may be sudden or gradual and can disrupt sleep.
- Intense pain with movement: Calcification decreases tendon contraction ability, reducing range of motion and causing stiffness.
- Tenderness over the rotator cuff: Associated with decreased movement and possible muscle atrophy.
How is Calcific Tendonitis Diagnosed?
Your physician will take a medical history and perform a physical exam. You may be referred to an orthopaedic specialist. Tests may include:
- Evaluation of shoulder range of motion and stability
- X-ray to detect calcific deposits
- MRI and radiography to assess soft tissues
Treatment
Most calcific deposits resorb naturally, but some patients require treatment for severe pain or persistent symptoms.
Physical Therapy
Sports physical therapy and massage promote muscle relaxation, decrease pain, and improve blood supply. Rehabilitation restores normal movement.
Medical Treatment
Painkillers such as NSAIDs (ibuprofen, naproxen) are effective. Cortisone or steroid injections (4) can reduce pain and swelling.
Lavage Treatment
A needle is placed into the shoulder and saline is injected to break up and flush out calcium deposits.
Extracorporeal Shock Wave Therapy (ESWT)
ESWT (5) uses mechanical shock waves to break up calcium deposits. Higher frequency shocks are more effective.
Radial Shock Wave Therapy (RSWT)
Similar to ESWT, RSWT delivers low- to medium-energy shocks to break up calcium deposits.
Therapeutic Ultrasound
High-frequency sound waves break down calcium deposits. This is usually painless (6).
Shoulder Barbotage
Dissection of calcium deposits using ultrasound guidance, often under local anesthesia.
Prolotherapy
In recent years, Prolotherapy has built its reputation within the medical community for its clinically proven ability to treat calcific tendonitis shoulder. Published research has proven its pain-relieving, anti-inflammatory and regenerative benefits. Prolotherapy involves injecting a natural regenerative solution with tiny needles. This has been shown to stimulate the production of collagen cells, the small cells needed to help with calcific tendonitis shoulder. As prolotherapy is helping to treat the root cause of calcific tendonitis shoulder, it is deemed to be a permanent fix, preventing the symptoms from returning.
 Disclaimer: The information provided in this section is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Prolotherapy may not be suitable for everyone, and outcomes can vary. Always seek the guidance of a qualified healthcare professional regarding your specific medical condition or treatment options. Never disregard professional medical advice or delay seeking it because of information you have read here.
Disclaimer: The information provided in this section is for educational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Prolotherapy may not be suitable for everyone, and outcomes can vary. Always seek the guidance of a qualified healthcare professional regarding your specific medical condition or treatment options. Never disregard professional medical advice or delay seeking it because of information you have read here.
Surgical Treatment
Surgery is reserved for severe cases and is usually considered after six months of failed conservative treatment. Surgery may be open or arthroscopic. Most surgeries are arthroscopic, using an arthroscope to locate and remove calcium deposits. Risks include infection, recurrence, and chronic pain.
Rehabilitation After Surgery
Rehabilitation can take weeks to months. Early movement is encouraged, but must be balanced with tissue protection. Therapy includes range-of-motion, strengthening, and stretching exercises. A therapist will guide you to avoid overuse and prevent future problems.
Preventive Measures
- Avoid heavy lifting and overhead activities.
- Warm up and stretch before exercise.
- Maintain healthy thyroid function and monitor for metabolic conditions like diabetes.
- Exercise regularly, but avoid overexertion.
Frequently Asked Questions
How effective is surgery compared to other options for shoulder calcific tendonitis?
Research shows no significant difference in outcomes between surgery and non-surgical treatments. Surgery should be considered only after conservative therapies like injections and shockwave therapy.
Should you undergo shockwave therapy for calcific tendonitis?
Shockwave therapy is as effective as injections, though it may take longer. High-energy shockwaves are more effective than low-energy ones.
Is your food a cause of calcific tendonitis of the shoulder?
Diet is not a direct cause, but obesity and diabetes can increase pain severity.
Will calcific tendonitis resolve on its own?
Most cases resolve without treatment, but persistent symptoms should be evaluated by a healthcare professional.
Can calcific tendinitis come back?
Symptoms can recur, especially in those with a history of arthritis or tendon tears. Regular checkups are recommended.
Contact ProHealth Clinic Today for Your FREE 15-Minute Discovery Call
Don’t let calcific tendonitis shoulder control your life any longer. Join the thousands of patients who have found lasting relief through prolotherapy at ProHealth Clinic.
Get in Touch
- Phone: +441234380345
- Email: info@prohealthclinic.co.uk
Our Clinic Locations
- London: 104 Harley Street, Marylebone, W1G 7JD
- Manchester: The Hadley Clinic, 64 Bridge Street, M3 3BN
- Bedford: The Village Medical Centre, Kingswood Way, MK40 4GH
All clinics offer the same award-winning prolotherapy treatment with convenient appointment times, including evenings and weekends.
Author Bio
Having performed over 10,000 procedures, Mr Oliver Eaton is one of the UK’s leading practitioners in the field of treating calcific tendonitis shoulder, with patients travelling to see him from across the UK, Europe, and the Middle East.
With over 12 years of clinical experience, Oliver is dedicated to helping patients understand their symptoms associated with calcific tendonitis shoulder and providing effective treatment options to alleviate them.
He qualified in Prolozone Therapy and Prolotherapy in America with the American Academy of Ozonotherapy. He continued on to complete further qualifications at the Royal Society of Medicine, Charing Cross Hospital in London, Keele University’s Anatomy & Surgical Training Centre, and the medical department of Heidelberg University in Germany.
Over the years he has had the privilege of treating many elite-level athletes, including both Olympic and Commonwealth medallists.
Mr Eaton’s expertise has been featured in many national news and media publications, including The Telegraph, The Daily Mail, The Daily Express, Women’s Health Magazine, and The Scotsman.
References
- Gärtner, J., & Heyer, A. (1995). Calcific tendonitis of the shoulder. Der Orthopade, 24(3), 284–302. https://europepmc.org/article/med/7617385
- Lui, P. P. Y. (2017). Calcific Tendonitis in diabetes mellitus patients—Epidemiology, pathogenesis, and management. Scandinavian Journal of Medicine & Science in Sports, 27(8), 776–787. https://doi.org/10.1111/sms.12824
- Darrieutort-Laffite, C., Blanchard, F., & Le Goff, B. (2018). Calcific tendonitis of the rotator cuff: From formation to resorption. Joint Bone Spine, 85(6), 687–692. https://doi.org/10.1016/j.jbspin.2017.10.004
- Gaujoux-Viala, C., Dougados, M., & Gossec, L. (2008). Efficacy and safety of steroid injections for shoulder and elbow tendonitis: a meta-analysis of randomized controlled trials. Annals of the Rheumatic Diseases, 68(12), 1843–1849.
Disclaimer: This article is for informational purposes only and does not substitute for professional medical advice. Always consult your healthcare provider before making treatment decisions.