Author: Mr Oliver Eaton BSc (Hons), PG.Cert – Orthopaedic Specialist
Reviewed by: Mr William Sharples BSc (Hons) – Pain Management Expert
Last Updated: September 2025
In this article, you will find out everything you need to know about osteomyelitis and the most effective ways to treat it
Osteomyelitis is a severe infection of the bone that can lead to significant complications if not addressed promptly. Osteomyelitis is an infection of the bone, most commonly a bacterial infection. This condition is often caused by bacteria or fungi entering the bone tissue, typically following an injury or surgical procedure. Key risk factors include older adults, diabetes, vascular insufficiency, sickle cell disease, and recent surgery. Infection spreads to the underlying bone via the bloodstream (hematogenous osteomyelitis), from adjacent tissues (contiguous osteomyelitis), or by direct inoculation such as a puncture wound or surgical site. Infected prosthesis and bone joint surg are important considerations in clinical practice. If not treated promptly, permanent bone loss and necrotic bone can occur as complications. Understanding the causes, symptoms, and available treatments is crucial for effective management of osteomyelitis.
Introduction to Osteomyelitis
Osteomyelitis is a serious infection that affects the bone and its surrounding structures. This condition can develop suddenly (acute osteomyelitis) or persist over time (chronic osteomyelitis), and is most often caused by bacteria, but can also result from fungi or mycobacteria. The infection may reach the bone through the bloodstream, following a fracture, or after surgical procedures. Osteomyelitis can affect people of any age and can involve any bone in the body. Early treatment is crucial, as delaying care increases the risk of permanent bone damage, abscess formation, and even life-threatening complications like sepsis. Recognizing the signs and seeking prompt medical attention can make a significant difference in outcomes and help preserve healthy bones.
Causes of Bone Infection (Osteomyelitis)
Osteomyelitis is primarily caused by bacterial infections, with Staphylococcus aureus being the most common culprit. Staphylococcus bacteria are the most common cause, but aerobic gram negative bacilli are also important, especially in adults.
The infection can occur when bacteria enter the body through open wounds, surgical sites, or the bloodstream. A puncture wound or surgical site can introduce bacteria directly to the underlying bone.
After entering the bloodstream, urinary tract infection and other systemic infections can lead to hematogenous osteomyelitis, especially in older adults.
Individuals with compromised immune systems, diabetes, or recent bone injuries are at increased risk. Sickle cell disease, vascular insufficiency, and infected prosthesis are additional risk factors.
Infection spreads either through the bloodstream (hematogenous osteomyelitis), from adjacent soft tissue (contiguous osteomyelitis), or direct inoculation.
Long bones are commonly affected in children, while spinal infections are more common in adults.
Compromised blood flow and blood supply can impair immune response and increase susceptibility to bone infection.
Bone joint surg can be a source of infection if proper precautions are not taken.
Symptoms of Osteomyelitis
Symptoms of osteomyelitis include severe pain in the underlying bone, swelling, redness, and warmth over the affected area. Affected area redness is a key sign of infection. Patients may also experience fever, fatigue, and a general feeling of unwellness. Vertebral osteomyelitis may present with chronic back pain. In chronic cases, necrotic bone and new bone formation may be seen. Elevated inflammatory markers such as CRP and ESR are often present and support the diagnosis. Early diagnosis and treatment are essential to prevent the infection from spreading and causing further damage.
Diagnosing Osteomyelitis

Diagnosing osteomyelitis requires a thorough approach that combines clinical assessment with advanced testing. Blood tests, such as a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP), are used to detect infection and inflammation in the body. Blood cultures can help identify the specific bacteria responsible for the bone infection, guiding targeted treatment. Imaging studies, including X-rays, magnetic resonance imaging (MRI), and computed tomography (CT) scans, provide detailed views of the affected bone and surrounding tissue, helping to detect osteomyelitis early and assess the extent of the infection. In some cases, a bone biopsy—removing a small sample of the affected bone for laboratory analysis—is necessary to confirm the diagnosis and determine the best course of treatment. For patients with diabetic foot infections, the probe-to-bone test can be a useful screening tool, though it is not definitive. Accurate diagnosis is essential for effective management and recovery.
Potential Complications of Osteomyelitis
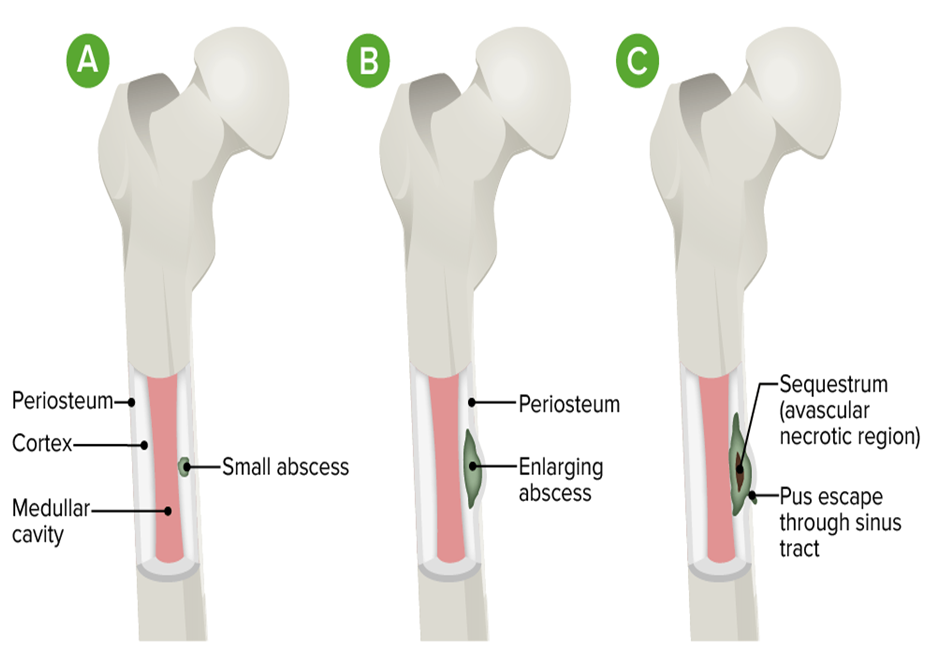
If osteomyelitis is not treated promptly and effectively, it can lead to a range of serious complications. Chronic osteomyelitis may develop, resulting in ongoing bone pain, persistent symptoms of osteomyelitis, and the risk of permanent bone damage. The infection can spread to nearby joints, causing septic arthritis, or extend into the soft tissue, leading to soft tissue infection and abscess formation. Other potential complications include the development of a sinus tract (an abnormal channel from the bone to the skin), bone deformity, and even systemic infections that can threaten overall health. In rare cases, chronic infection can increase the risk of certain cancers, such as squamous cell carcinoma, or lead to amyloidosis. Severe or untreated cases may result in disability, decreased quality of life, or the need for amputation. Recognizing symptoms like bone pain, swelling, redness, and warmth over the affected area is vital for early intervention and preventing these complications.
Antibiotic Treatment and Other Treatments for Osteomyelitis
Treatment for osteomyelitis typically involves a combination of antibiotics to eliminate the infection, often administered intravenously for several weeks. The antibiotic course usually lasts 4-6 weeks and is tailored to the causative organism.
In some cases, surgical intervention may be necessary to remove infected tissue or bone. Bone joint surg may be required to remove necrotic bone or an infected prosthesis, and careful management of the surgical site is essential for optimal recovery.
In clinical practice, osteomyelitis is treated according to established guidelines to prevent permanent bone loss. Treatment decisions are guided by how osteomyelitis is diagnosed, including laboratory and imaging findings. Early and aggressive treatment is crucial to prevent chronic infection and complications.
Prevention and Management
Preventing osteomyelitis starts with good hygiene practices, especially after injuries or surgical procedures, to reduce the risk of bone infections. Managing chronic conditions such as diabetes mellitus and supporting a healthy immune system are also important steps in lowering the risk of developing osteomyelitis. When a bone infection is suspected, prompt antibiotic treatment is essential to control the infection and prevent further damage. The choice of antibiotics depends on the type of bacteria involved and the severity of the infection. In some cases, surgical debridement is necessary to remove dead bone and infected tissue, helping to restore healthy bone formation and prevent the spread of infection. Completing the full course of prescribed antibiotics is crucial to avoid complications and reduce the risk of antibiotic resistance. By taking these preventive and management steps, individuals can significantly decrease their chances of developing or worsening osteomyelitis.
Care and Recovery
Effective care and recovery from osteomyelitis require a comprehensive approach. Patients should follow their healthcare provider’s instructions closely, including taking all prescribed antibiotics and attending regular follow-up appointments to monitor progress. In some cases, intravenous antibiotic therapy may be needed, either in the hospital or as an outpatient. Maintaining a healthy lifestyle—such as eating a balanced diet, getting regular exercise, and ensuring adequate rest—can support the immune system and promote healing. For those recovering at home, proper wound care and dressing changes are important to prevent reinfection. With diligent care and adherence to antibiotic therapy, most people with osteomyelitis can achieve full recovery and return to their normal activities. However, it is important to remain vigilant for any signs of complications and seek medical attention if symptoms persist or worsen.
Case Study: Successful Management of Chronic Osteomyelitis
Patient: Male, 45, construction worker
Symptoms: Persistent bone pain, swelling, and fever following a leg injury.
Treatment: Osteomyelitis was diagnosed using imaging and laboratory tests. The patient completed a full antibiotic course and underwent surgical debridement of necrotic bone at the surgical site at ProHealth Clinic.
Outcome: Within three months, the patient experienced significant pain reduction and improved mobility, with no signs of infection at the one-year follow-up. The osteomyelitis was successfully treated, with no recurrence at follow-up.
Frequently Asked Questions
What is the most effective treatment for osteomyelitis?
The most effective treatment often involves a combination of antibiotics and, in some cases, surgery. Osteomyelitis is treated according to clinical practice guidelines, and it is essential to diagnose osteomyelitis accurately to guide therapy. Early intervention is key to successful outcomes.
Can osteomyelitis be cured completely?
With prompt and appropriate treatment, osteomyelitis can be effectively managed and cured. If the infection persists or recurs, it is called chronic osteomyelitis. However, chronic cases may require long-term management strategies. Preventive measures, such as good wound care and managing chronic diseases, can help prevent osteomyelitis.
Is surgery always necessary for osteomyelitis?
Surgery is not always necessary but may be required to remove infected tissue or bone, especially in severe cases. Your healthcare provider will determine the best course of action based on your specific condition. A thorough differential diagnosis is important to determine whether surgery is needed for osteomyelitis or another condition.
Contact ProHealth Clinic Today for Your FREE 15-Minute Discovery Call
Don’t let osteomyelitis control your life any longer. Join the thousands of patients who have found lasting relief through prolotherapy at ProHealth Clinic.
Get in Touch
Phone: +441234380345
Email: info@prohealthclinic.co.uk
Our Clinic Locations
London: 104 Harley Street, Marylebone, W1G 7JD
Manchester: The Hadley Clinic, 64 Bridge Street, M3 3BN
Bedford: The Village Medical Centre, Kingswood Way, MK40 4GH
All clinics offer the same award-winning prolotherapy treatment with convenient appointment times, including evenings and weekends.
Author Bio
Having performed over 10,000 procedures, Mr Oliver Eaton is one of the UK’s leading practitioners in the field of treating osteomyelitis, with patients travelling to see him from across the UK, Europe, and the Middle East.
With over 12 years of clinical experience, Oliver is dedicated to helping patients understand their symptoms associated with osteomyelitis and providing effective treatment options to alleviate them.
He qualified in Prolozone Therapy and Prolotherapy in America with the American Academy of Ozonotherapy. He continued on to complete further qualifications at the Royal Society of Medicine, Charing Cross Hospital in London, Keele University’s Anatomy & Surgical Training Centre, and the medical department of Heidelberg University in Germany.
Over the years he has had the privilege of treating many elite-level athletes, including both Olympic and Commonwealth medallists.
Mr Eaton’s expertise has been featured in many national news and media publications, including The Telegraph, The Daily Mail, The Daily Express, Women’s Health Magazine, and The Scotsman.
References
- Lew DP, Waldvogel FA. Osteomyelitis. Lancet. 2004;364(9431):369-379. View Study
- Calhoun JH, Manring MM. Adult osteomyelitis. Infect Dis Clin North Am. 2005;19(4):765-786. View Study
- Trampuz A, Zimmerli W. Diagnosis and treatment of infections associated with fracture-fixation devices. Injury. 2006;37 Suppl 2:S59-66. View Study
Disclaimer: This article is for informational purposes only and does not substitute for professional medical advice. Always consult your healthcare provider before making treatment decisions.